International
ADVANCED AND APPLIED SCIENCES
EISSN: 2313-3724, Print ISSN: 2313-626X
Frequency: 12
![]()
Volume 9, Issue 7 (July 2022), Pages: 65-73

----------------------------------------------
Original Research Paper
Beneficial effects of RAS blockers in prediabetics with a hypertension-An observational cohort study
Author(s): Manika Bose 1, *, Tapaswini Mishra 2, Debasish Misra 1, Smita Das 1, Swati Mishra 1, Sudhanshu Sekhar Mishra 1
Affiliation(s):
1Department of Pharmacology, IMS and SUM Hospital, Siksha ‘O’ Anusandhan University, Bhubaneswar, Odisha, India
2Department of Physiology, IMS and SUM Hospital, Siksha ‘O’ Anusandhan University, Bhubaneswar, Odisha, India

* Corresponding Author.
 Corresponding author's ORCID profile: https://orcid.org/0000-0002-0848-0315
Corresponding author's ORCID profile: https://orcid.org/0000-0002-0848-0315
Digital Object Identifier:
https://doi.org/10.21833/ijaas.2022.07.008
Abstract:
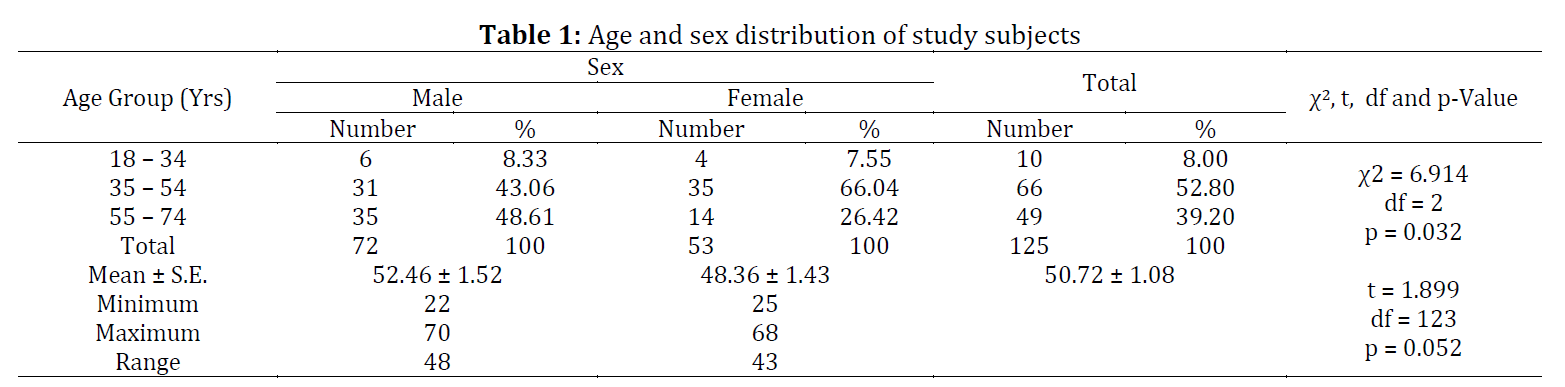
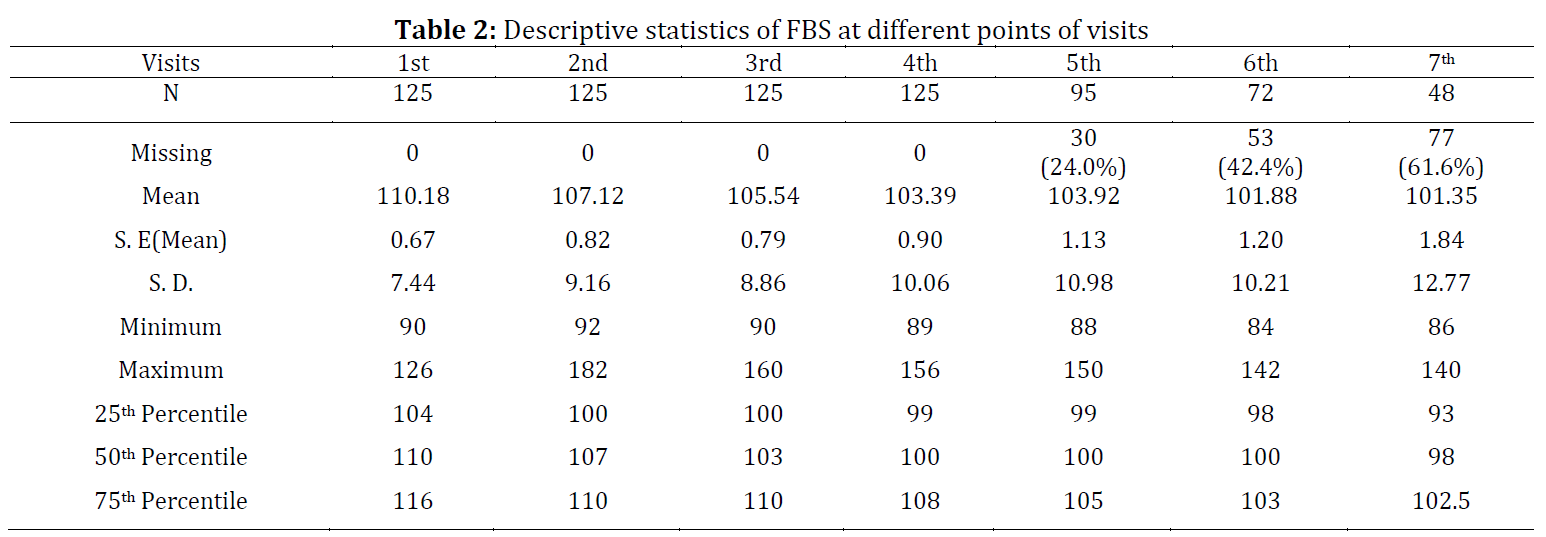
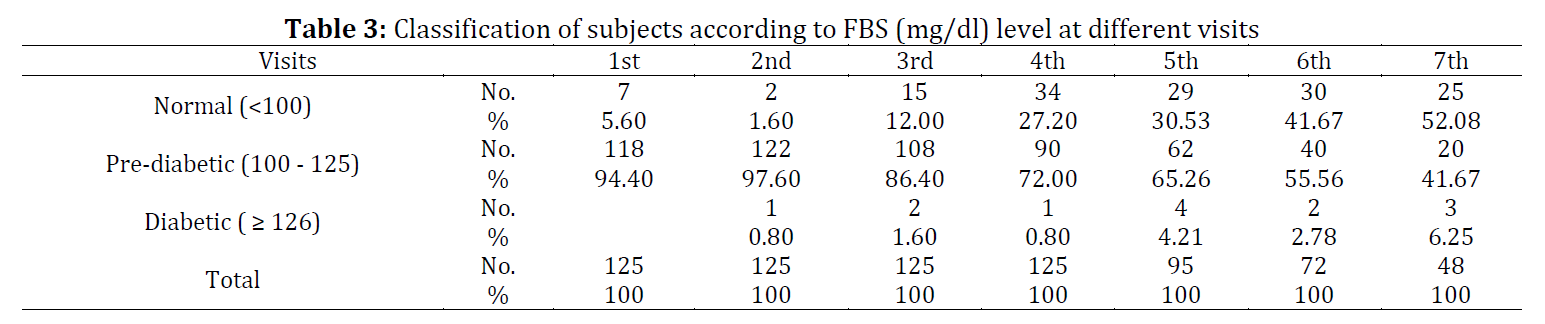
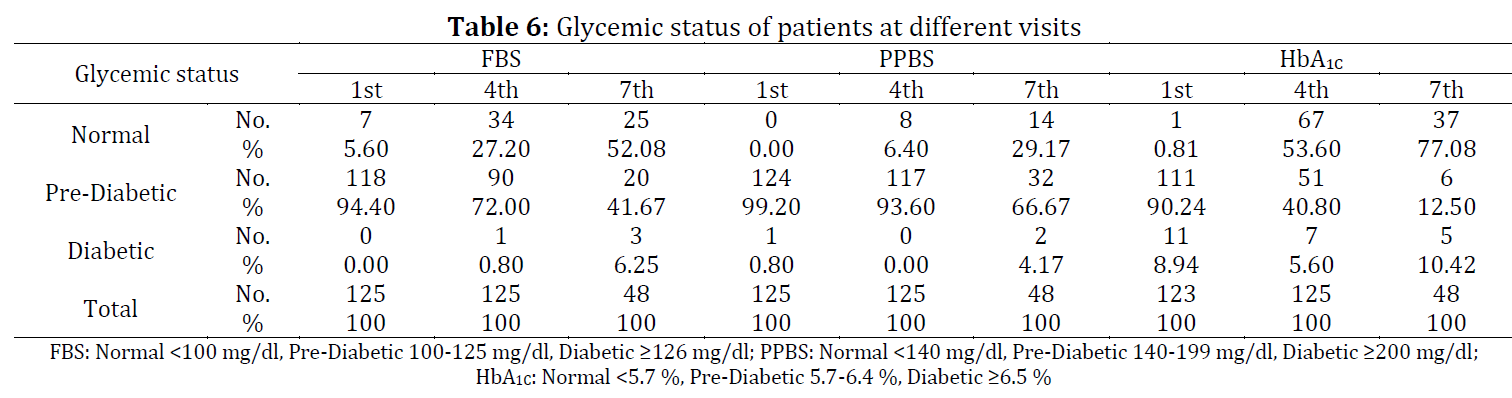
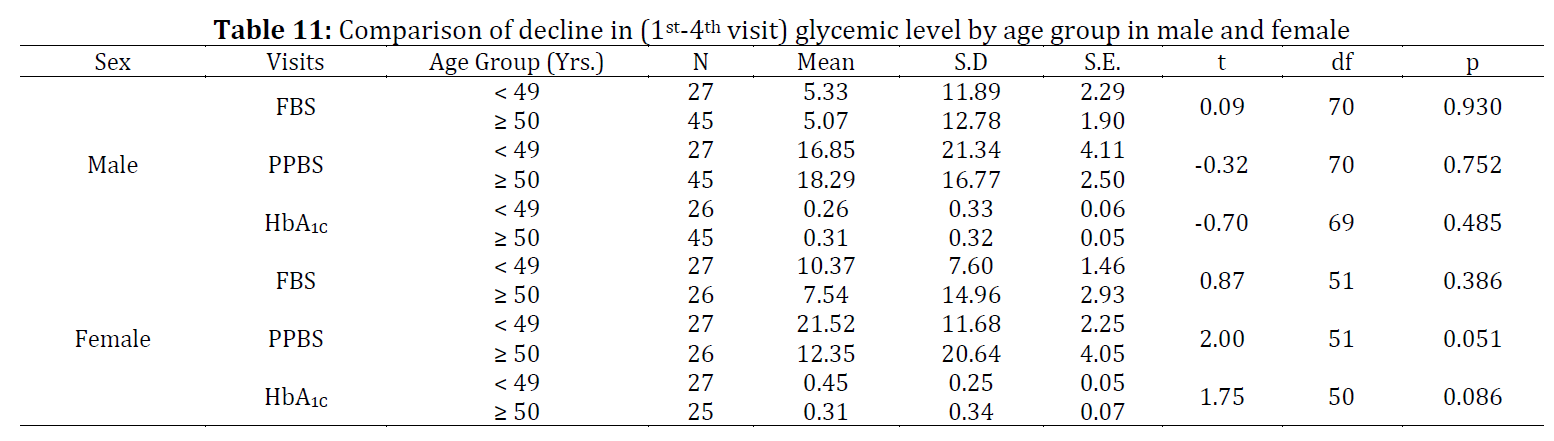
Hypertensive patients have a high prevalence of prediabetes and type II Diabetes mellitus. As per International Diabetic Federation, it has been estimated that more than 470 million people will have prediabetes by 2030. Approximately 5-10% of prediabetes progresses to overt diabetes mellitus, with the same proportion converting back to normoglycemia. In patients who are on Renin-Angiotensin System [RAS] blockers either an Angiotensin converting enzyme inhibitor (ACEI) or an Angiotensin receptor blocker (ARB) would slow down the progress of prediabetic state to overt or frank diabetes mellitus. This was a prospective, observational cohort study and a total of 125 hypertensive patients with impaired glucose tolerance were included in the study who were either on ACE inhibitor or ARB monotherapy. An oral Glucose Tolerance Test (GTT) was done at baseline for screening prediabetic patients, then a periodical assessment of glycemic indices, (fasting blood sugar, 2 hr postprandial blood sugar, and glycosylated hemoglobin), lipid profile, and complication status during the study period were evaluated every 3 months for18months. At the end of 1½ years, for patients belonging to the age group 18-54 years the FBS, PPBS, and HbA1C levels decreased significantly when the RAS blocking drugs (ACEIs and ARBs) were used continuously for 1 year and then they got stabilized. The beneficial effect was seen more in the younger age group 18-54 years old patients. Male above 54 years and females above 49 were resistant to the beneficial effects. In hypertensive patients with impaired glucose tolerance, the blockade of RAS with either ACE inhibitor or ARB has a significant preventive effect on the progression of Type II DM. It may be concluded from the finding of the present study that younger hypertensive patients (18-54 years) of either sex if found to be pre-diabetic may be administered ACEI or ARB as suitable for them. The treatment should be continued vigorously for one year and then it may be maintained to continue the beneficial effect.
© 2022 The Authors. Published by IASE.
This is an
Keywords: Prediabetes, Renin angiotensin system blockade, Age, Impaired glucose tolerance
Article History: Received 29 November 2021, Received in revised form 17 April 2022, Accepted 20 April 2022
Acknowledgment
The authors wish to thank all the participants who supported the research.
Compliance with ethical standards
Ethical considerations: Our study design was approved by the Institutional Ethical Committee Hospital, Letter no-IMS SH/IEC/2013/44.
Conflict of interest: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Citation:
Bose M, Mishra T, and Misra D et al. (2022). Beneficial effects of RAS blockers in prediabetics with a hypertension-An observational cohort study. International Journal of Advanced and Applied Sciences, 9(7): 65-73
Figures
{kind=link}
Tables
Table 1 Table 2 Table 3 Table 4 Table 5 Table 6 Table 7 Table 8 Table 9 Table 10 Table 11
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
----------------------------------------------
References (21)
- Arauz-Pacheco C, Parrott MA, and Raskin P (2003). Treatment of hypertension in adults with diabetes. Diabetes Care, 26: S80-82. https://doi.org/10.2337/diacare.26.2007.S80 [Google Scholar] PMid:12502624
- Beverley B and Eschwège E (2003). The diagnosis and classification of diabetes and impaired glucose tolerance. In: Pickup JC and Williams G (Eds.), Textbook of diabetes, 1: 21-211. 3rd Edition, John Wiley and Sons, Hoboken, USA. [Google Scholar]
- Bhalla N, Mohan G, Kaur R, and Bansal K (2013). To study the prevalence of impaired fasting glucose and its correlation with various anthropometric variables. Journal of Evolution of Medical and Dental Sciences, 2(52): 10158-10164. https://doi.org/10.14260/jemds/1750 [Google Scholar]
- Califf RM, Boolell M, Haffner SM, Bethel MA, McMurray J, Duggal A, and Holman RR (2008). Prevention of diabetes and cardiovascular disease in patients with impaired glucose tolerance: Rationale and design of the Nateglinide and Valsartan in impaired glucose tolerance outcomes research (NAVIGATOR) trial. American Heart Journal, 156(4): 623-632. https://doi.org/10.1016/j.ahj.2008.05.017 [Google Scholar] PMid:18946890
- Conroy RM, Pyörälä K, Fitzgerald AE, Sans S, Menotti A, De Backer G, and Graham IM (2003). Estimation of ten-year risk of fatal cardiovascular disease in Europe: The score project. European Heart Journal, 24(11): 987-1003. https://doi.org/10.1016/S0195-668X(03)00114-3 [Google Scholar]
- Dahlöf B, Sever PS, Poulter NR, Wedel H, Beevers DG, Caulfield MM, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, and Mehlsen J (2005). Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): A multicentre randomised controlled trial. The Lancet, 366(9489): 895-906. https://doi.org/10.1016/S0140-6736(05)67185-1 [Google Scholar]
- Ferrannini E, Gastaldelli A, Miyazaki Y, Matsuda M, Pettiti M, Natali A, and DeFronzo RA (2003). Predominant role of reduced beta-cell sensitivity to glucose over insulin resistance in impaired glucose tolerance. Diabetologia, 46(9): 1211-1219. https://doi.org/10.1007/s00125-003-1169-6 [Google Scholar] PMid:12879253
- Gress TW, Nieto FJ, Shahar E, Wofford MR, and Brancati FL (2000). Hypertension and antihypertensive therapy as risk factors for type 2 diabetes mellitus. New England Journal of Medicine, 342(13): 905-912. https://doi.org/10.1056/NEJM200003303421301 [Google Scholar] PMid:10738048
- Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, and Sowers JR (1999). Diabetes and cardiovascular disease: A statement for healthcare professionals from the American Heart Association. Circulation, 100(10): 1134-1146. https://doi.org/10.1161/01.CIR.100.10.1134 [Google Scholar] PMid:10477542
- Hansson L, Lindholm LH, Niskanen L, Lanke J, Hedner T, Niklason A and Björck JE (1999). Effect of angiotensin-converting-enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: The captopril prevention project (CAPPP) randomised trial. The Lancet, 353(9153): 611-616. https://doi.org/10.1016/S0140-6736(98)05012-0 [Google Scholar]
- Ibrahim MM (2006). RAS inhibition in hypertension. Journal of Human Hypertension, 20(2): 101-108. https://doi.org/10.1038/sj.jhh.1001960 [Google Scholar] PMid:16397519
- Jandeleit-Dahm KA, Tikellis C, Reid CM, Johnston CI, and Cooper ME (2005). Why blockade of the renin–angiotensin system reduces the incidence of new-onset diabetes. Journal of Hypertension, 23(3): 463-473. https://doi.org/10.1097/01.hjh.0000160198.05416.72 [Google Scholar] PMid:15716683
- Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, and Plat F (2004). Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: The VALUE randomised trial. The Lancet, 363(9426): 2022-2031. https://doi.org/10.1016/S0140-6736(04)16451-9 [Google Scholar]
- Kumar PJ Clark M (2002). Textbook of clinical medicine. 8th Edition, Saunders, London, UK. [Google Scholar]
- Masiá R, Sala J, Rohlfs I, Piulats R, Manresa JM, and Marrugat J (2004). Prevalence of diabetes mellitus in the province of Girona, Spain: The REGICOR study. Revista Española de Cardiología (English Edition), 57(3): 261-264. https://doi.org/10.1016/S1885-5857(06)60145-X [Google Scholar]
- Nichols GA, Hillier TA, and Brown JB (2007). Progression from newly acquired impaired fasting glusose to type 2 diabetes. Diabetes Care, 30(2): 228-233. https://doi.org/10.2337/dc06-1392 [Google Scholar] PMid:17259486 PMCid:PMC1851903
- Padwal R and Laupacis A (2004). Antihypertensive therapy and incidence of type 2 diabetes: A systematic review. Diabetes Care, 27(1): 247-255. https://doi.org/10.2337/diacare.27.1.247 [Google Scholar] PMid:14693997
- Ruilope LM and Segura J (2003). Losartan and other angiotensin II antagonists for nephropathy in type 2 diabetes mellitus: A review of the clinical trial evidence. Clinical Therapeutics, 25(12): 3044-3064. https://doi.org/10.1016/S0149-2918(03)90091-9 [Google Scholar]
- Scheen A (2006). Etude clinique du mois: L'etude DREAM: Prevention du diabete de type 2 par le ramipiril et/ou la rosiglitazone chez les personnes dysglycemiques sans maladie cardio-vasculaire. Revue Médicale de Liège, 61(10): 728-732. [Google Scholar]
- Unwin N, Shaw J, Zimmet P, and Alberti KG (2002). Impaired glucose tolerance and impaired fasting glycaemia: The current status on definition and intervention. Diabetic Medicine: A Journal of the British Diabetic Association, 19(9): 708-723. https://doi.org/10.1046/j.1464-5491.2002.00835.x [Google Scholar] PMid:12207806
- Yang W, Lu J, Weng J, Jia W, Ji L, Xiao J, and He J (2010). Prevalence of diabetes among men and women in China. New England Journal of Medicine, 362(12): 1090-1101. https://doi.org/10.1056/NEJMoa0908292 [Google Scholar] PMid:20335585